As Cerenkov luminescence imaging and similar techniques find their way into clinical use, molecular imaging arrives in the cancer operating room.
KUNAL VYAS, LIGHTPOINT MEDICAL LTD.
Molecular imaging has become an invaluable tool in cancer treatment. Single-photon emission computed tomography (SPECT) and positron emission tomography (PET) are entering routine clinical use for preoperative imaging. These techniques visualize cancerous tissue by measuring the biodistribution of a radiotracer that specifically targets cancer cells.
Molecular scans are essential for diagnosing cancer and planning surgical interventions. In the operating room, however, surgeons still rely on sight and touch to ensure that all cancerous tissue is removed and that as much healthy tissue is spared as possible. The removal of all of the cancer during surgery is critical because leaving cancerous tissue behind may allow the disease to persist, requiring further treatment. Surgeons also seek to avoid removing healthy tissue, the loss of which can impair physiological function and lead to negative long-term outcomes for the patient.
Currently, approximately one in four prostate cancer patients and one in five breast cancer patients leave the operating room with cancer tissue remaining, prompting an urgent medical need for tools to more accurately detect the location of cancer during surgery.
Systems for preoperative imaging such as SPECT and PET cannot be employed within the time and space restrictions of an operating room. However, it is possible to use an optical camera. The Cerenkov effect — whereby light is produced if a charged particle from a radiotracer, which accumulates in cancerous tissue, travels faster than light travels through the tissue — makes optical imaging possible. The technique, called Cerenkov luminescence imaging (CLI), is used by Lightpoint Medical and their intraoperative molecular imaging device, LightPath.
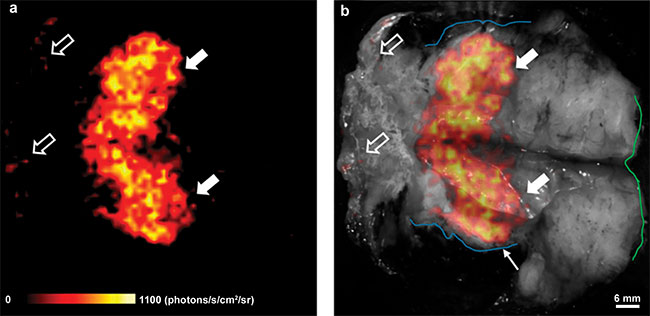
Figure 1. Wide, local excision specimen (removed tumor) from a patient with breast cancer. In this case, the specimen was partially dissected, revealing the
central cancerous tissue. The line of dissection is seen horizontally, resulting in the symmetric appearance of the image. Cerenkov image (a); gray-scale photographic image overlaid with Cerenkov signal (b). An increased signal from the tumor is visible (white arrows); mean radiance is 871 ± 131 photons/s/cm2/sr. Surgeons measured the posterior margin (outlined in blue) as 2 mm (small arrow). The medial margin (outlined in green) measured >5 mm by both surgeons. Pathology ink prevented assessing the lateral margin; a phosphorescent signal is visible (open arrows). Adapted from reference 1 on page 47.
Prior to surgery, the patient is injected with a cancer-targeting radiopharmaceutical that then selectively accumulates in cancerous tissue. LightPath can scan excised tumor specimens during surgery. The device is designed to rapidly visualize the distribution of the radiotracer in the surface layer of the specimen. This helps the surgeon determine whether the surgical margin is clear or more tissue needs to be removed. The first intraoperative clinical measurements for breast cancer surgery were reported in 20161 (Figure 1). A 150-patient multicenter trial in breast cancer (post-market study) — as well as investigations into several other applications, including prostate, and head and neck — is ongoing.
Why CLI?
The detection mechanisms between PET and CLI differ; however, the same positron-emitting radioisotopes are detected, including flourine-18 (18F) and gallium-68 (68Ga). An important distinction between the two techniques (Figure 2) is that the gamma photons detected by PET penetrate through the tissue, unlike with the optical Cerenkov photons required for CLI. These are scattered and absorbed as they travel in the tissue, and only those generated close to the surface escape; therefore, CLI cannot replace PET preoperative imaging. Because of its high surface specificity, lower cost, smaller footprint, and shorter acquisition times, CLI is more suitable for inspecting margins during surgery.
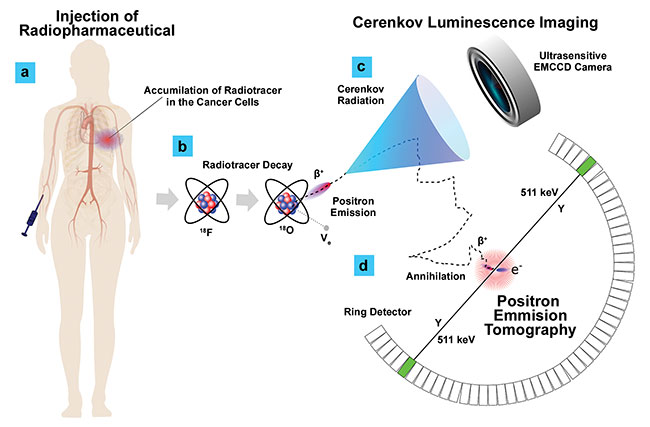
Figure 2. The principle of Cerenkov and PET imaging using positron-emitting radiopharmaceuticals. A radiopharmaceutical, for example 18F-fludeoxyglucose (18F-FDG), is administered systemically (a). 18F-FDG is a glucose analog and therefore accumulates in cancer cells on account of their hypermetabolism. The uptake in cancer cells and clearance from healthy tissue requires approximately 2 h. The 18F undergoes radioactive decay (b) with a half-life of 110 mins and emits positrons (β+) with up to 633.5 keV of kinetic energy. As a result of the refractive index of tissue, at energies greater than 220 keV the positrons are traveling faster than light can travel through the tissue (c). This triggers an “optical boom,” and the particles emit Cerenkov photons at visible wavelengths; these photons are utilized for CLI. The positron continues its journey, quickly losing energy through scattering and then being annihilated when it collides with an electron in the tissue, releasing two 511 keV gamma photons (d). The gamma photons travel in opposition to each other and can be detected by a PET detector ring. The small difference in arrival times can be used to reconstruct the point of origin of each pair of photons to build a 3D map of the radiotracer distribution. Courtesy of Kunal Vyas/Lightpoint Medical.
Cerenkov emissions are extremely weak for clinical radioactivity concentrations and are heavily attenuated by tissue. Only a few photons per pixel are captured over 5 min using f/0.95 optics. The readout and dark noise from a conventional CCD or CMOS camera would overwhelm the Cerenkov signal. It is therefore necessary to use a high-gain, low-noise detector, such as a deep-cooled ultrasensitive electron-multiplying CCD (EMCCD), along with carefully designed instrumentation and image processing.
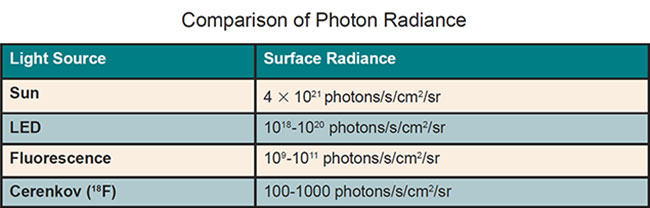
The table above demonstrates the challenging nature of the problem and shows a comparison of the photon radiance of various light sources compared to Cerenkov signals.
Fluorescence signals can be many orders of magnitude brighter, and they have the benefit of being flexible and relatively narrowband in wavelength, which allows better rejection of background using optical bandpass filters and lock-in techniques. Despite these advantages, fluorescence is not competitive in oncology surgery. There are no approved cancer-targeting fluorescence agents, and barriers include the prohibitive cost of developing novel agents and greater toxicity risk due to higher required dosages compared to radiopharmaceuticals. Radiotracers, such as 18F-FDG, however, have been in widespread use for decades and have accrued an extensive body of clinical evidence.
Enhanced detection methods
The spectrum and depth sensitivity of CLI in breast tissue — via the LightPath imaging system (Figure 3) — are surface-specific because of the attenuation of the Cerenkov radiation in tissue, making it ideal for surgical margin inspection.
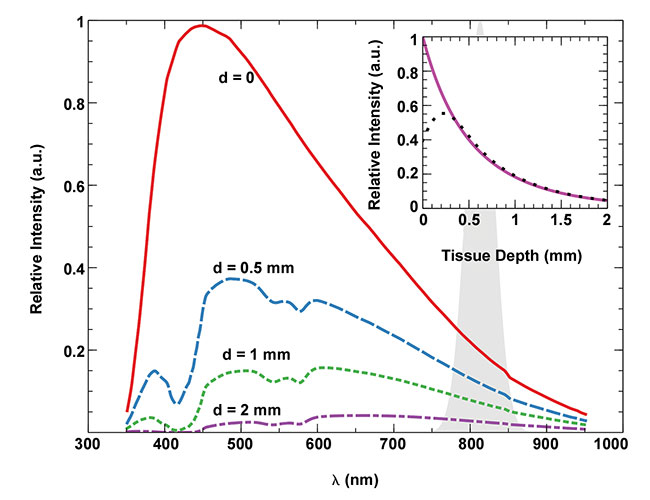
Figure 3. The expected spectrum of detected CLI signal from different depths of breast tissue. The intrinsic λ-2 Cerenkov radiation spectrum provided by the Frank-Tamm formula is modified by wavelength-dependent absorption and scattering in a generic breast tissue model (see reference 4) and the quantum efficiency curve of the LightPath imaging system. The unlabeled shaded peak at 813 nm indicates the comparatively narrow emission spectrum of indocyanine green (ICG), an untargeted fluorescent tracer generally used to visualize vasculature. The solid purple trace in the inset shows how the Cerenkov intensity quickly drops off with Cerenkov emission depth, resulting in a surface-specific signal. The black dotted line in the inset shows a similar depth dependence based on 18F decay depth. For decays that occur very close to the surface, some positrons can escape, which shortens the average track length in tissue and results in lower potential to emit Cerenkov radiation. Courtesy of Kunal Vyas/Lightpoint Medical.
The broadband nature of the Cerenkov signal, however, combined with the extremely low radiance, does pose a problem. It is not possible to filter out interferences — such as phosphorescence of the tissue or contaminants, optical emission due to thermal energy deposited by electrocautery devices, or ambient light leakage — without loss of precious signal. To address this challenge, the following three enhancements should be considered: an approved nonspecific fluorescent molecule to enhance the signal or present a narrowband target, a higher-energy-emitting isotope (for example, 68Ga) to boost signal levels, or a change in radiation detection method.
1. An approved nonspecific fluorescent molecule. The use of a fluorescence conversion is not currently a preferred clinical solution because the distribution of the untargeted fluorescent molecule modifies the resultant signal.
2. A higher-energy-emitting isotope. An attractive candidate for CLI is 68Ga because of the higher maximum positron emission energy of 1.92 MeV compared to 0.66 MeV for 18F. The compounding effects of an increase in the probability that positrons are released at sufficient energy to emit Cerenkov radiation in tissue (>220 keV), from 53 percent for 18F to 93 percent for 68Ga, leads to a >20× lowering of the detection limit2. So does an increase in the number of Cerenkov photons emitted by such positrons, thanks to higher average energies and longer average track lengths in the tissue. Because of its chemistry, 68Ga is not available for every target, and the higher energy leads to lower resolution and depth specificity.
3. A change in radiation detection method. The radiation detection method can be changed to detect the positrons that escape the tissue surface using a thin scintillator, such as the LightPath system accessory3. To maximize performance, such scintillators are flexible and conform to the specimen surface. This results in an improvement in depth specificity and increased sensitivity over standard CLI, particularly for low-energy isotopes such as 18F. The narrowband emission spectrum can also allow for filter-based rejection of interferences.
In summary, CLI and related techniques that leverage SPECT or PET radiotracers benefit from the availability of approved cancer-targeting agents with large bodies of clinical evidence from preoperative imaging. However, they face the challenge of achieving sufficient sensitivity and surface specificity.
Meet the author
Kunal Vyas, Ph.D., is the senior scientist at Lightpoint Medical Ltd., where he has helped develop the company’s core technologies. His role includes leadership of research toward Lightpoint’s next generation of products, as well as management of the company’s IP
portfolio; email: [email protected].
References
1. M. Grootendorst et al. (2016). Intraoperative assessment of tumor resection margins in breast-conserving surgery using 18F-FDG Cerenkov luminescence imaging: a first-
in-human feasibility study. J Nucl Med,
Vol. 59, Issue 12, pp. 891-898.
2. J. Heuvel et al. (2018). Performance evaluation of Cerenkov luminescence imaging: a comparison of 68Ga with 18F. J Nucl Med, Vol. 59, Issue 12, pp. 365.
3. K. Vyas et al. (2018). Flexible scintillator autoradiography for tumor margin inspection using 18F-FDG. Proc SPIE, Vol. 10478, Molecular-Guided Surgery: Molecules, Devices, and Applications IV, https://doi.org/10.1117/12.2289693.
4. S. Jacques et al. (2013). Optical properties of biological tissues: a review. Phys Med Biol, Vol. 58, Issue 11, pp. R37-R61.
Quest for More Effective Cancer Care
The prevalence of cancer is growing rapidly worldwide. This year, there will be over 18 million new cases, and the disease will account for around one in six deaths globally. By 2030, the incidence rate is set to soar by more than 60 percent, with over 24 million new cases each year1.
Surgery is one of the primary treatments for cancer. The aim is to remove a clear margin of noncancerous tissue around the circumference of the excised tumor, while sparing healthy, functional tissue. Numerous studies have demonstrated improved outcomes for cancer patients with a clear surgical margin status. Those that show inadequate margins require adjuvant treatments, including reoperations, radiotherapy, and chemotherapy, which can severely impact quality of life and add a considerable cost to health care systems.
Currently, oncology surgeons depend on sight and touch to determine surgical margins, which is extremely challenging, particularly because some tumors are not even visible to the naked eye and palpation is inaccurate. The tumor can be estimated preoperatively by CT and MRI images, but these do not provide sufficient information to guide accurate surgical excision. Only postoperative pathology tests can confirm whether a clear margin has been achieved. Approximately one in four prostate cancer patients and one in five breast cancer patients find out that they have inadequate surgical margins after surgery. In head and neck cancer, the figure is reported as high as 85 percent2.
A system such as Lightpoint Medical’s LightPath can image signals from radiopharmaceuticals that travel only a few millimeters in biological tissue, indicating positive signal from cancerous cells found only within a few millimeters of the tissue’s surface. This is ideal for surgical margin assessment, where adequate margins are generally defined as having no cancerous cells remaining within a few millimeters from the margin of excision. LightPath produces scans within a couple of minutes during surgery, providing images that will help guide a surgeon in real time. The device promises the accurate identi?cation and surgical removal of cancer, with significant potential improvements for cancer patients.
References
1. GLOBOCAN 2018, http://gco.iarc.fr/.
2. R.W. Smits et al. (2015). Resection margins in oral cancer surgery: room for improvement. Head Neck, Vol. 38, Issue S1, pp. E2197-2203, https://doi.org/10.1002/hed.24075.