While diode lasers have been used to treat epilepsy via tissue ablation for years, new laser techniques aim to stop the spread of seizure activity in the brain.
For decades, the most commonly used treatments for epilepsy were pharmaceuticals or resection surgery, which involves removing a segment of brain tissue from where the patient’s seizures originate. These remedies can work well and continue to be the best treatment option in many cases, but they can also cause debilitating side effects. For some patients, drug therapy has proven ineffective, leaving them searching for another solution. Modern laser therapy has been shown in both clinical and proof-of-concept studies to be potentially helpful or even curative for many, because of its unique ability to precisely target affected brain tissue and stop or at least minimize the erratic signals emanating from it.
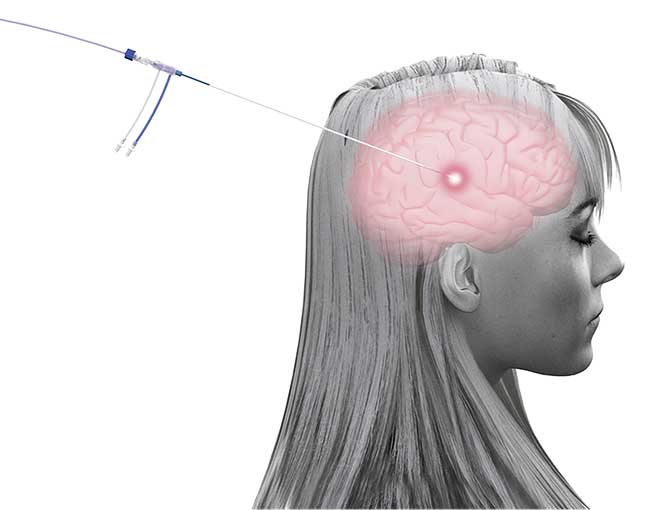
An illustration of the Visualase system connected to a patient’s brain. Courtesy of Medtronic.
An estimated 1.2% of the U.S. population has active epilepsy, and one in 26 people will develop it in their lifetime. Worldwide, according to the World Health Organization, as many as 50 million people have the neurological disorder. Generalized epilepsy is a condition in which an imbalance of excitatory and inhibitory neural connections can induce seizures throughout the brain. Focal epilepsy involves an imbalance that begins in one region of the brain and propagates to larger areas.
Epilepsy is usually diagnosed after a person experiences two or more seizures, without a known trigger, occurring more than 24 hours apart. Seizures cause brief, involuntary movements that may occur along with a loss of consciousness or other functioning.
Several forms of laser therapy, including ablation, have been used for over a decade to treat certain types of epilepsy. Ongoing research into the use of various types of lasers at particular wavelengths has revealed their potential for preventing the recurrence of seizures, which could allow those who suffer from them and haven’t been helped by other treatments to live normal lives.
An alternative to the scalpel
A team of researchers and clinicians at Cornell University has been experimenting with unique ways that pulsed lasers can be used to reduce and possibly eliminate seizures in animals1. While human clinical application is likely years away, the team is encouraged by the findings of its research so far.
“The standard curative treatment for focal epilepsy is resection, which can work well, but it can also produce permanent neurological deficits,” said Chris Schaffer, an associate professor in the Meinig School of Biomedical Engineering at Cornell.
Imaging methods have shown that most seizures spread laterally via subsurface lateral neural connections in specific cortical layers within the brain. Severing specific dysfunctional connections instead of resecting the entire epileptic focus could reduce the neurological deficits sometimes caused by epilepsy surgery. However, cutting subsurface neural connections is a procedure that cannot be performed with a mechanical scalpel.
“In our work, we wanted to create a precise laser scalpel and have laser pulses that could cut very sharply, deep within the tissue, without affecting the surrounding tissue,” Schaffer said.
He and the Cornell research team used a Ti:sapphire laser (Figure 1) emitting at 800 nm that generated 50-fs pulses to cut ~100-µm-wide subsurface cortical incisions, as deep as 1 mm, in rat neocortices. These incisions produced a “box” around a chemically induced epileptic focus that blocked seizure propagation.
Figure 1. The Ti:sapphire laser used by researchers at Cornell University in animal models to stop seizure propagation. Courtesy of Seth Lieberman/Cornell University.
Other neural signals entering and leaving the cortex — such as the neural signals required to coordinate the action of reaching for pellets or to feel sensations in the tail — were uninterrupted. Laser speckle imaging revealed that blood flow was also unaffected in the region incised with the laser.
Utilizing a model of acute seizures chemically induced by injecting iron chloride, researchers in Schaffer’s lab, including Seth Lieberman (Figure 2), were able to show that all seizure propagation was successfully blocked in one-third of the rats in the study. In other cases, seizure frequency or propagation was reduced. In the ongoing study, the researchers switched to the model of chronic seizures, and the results so far have surprised them. They were able to increase the efficiency of the laser cuts, blocking upward of 80% of chronic seizure propagation in rats for months.
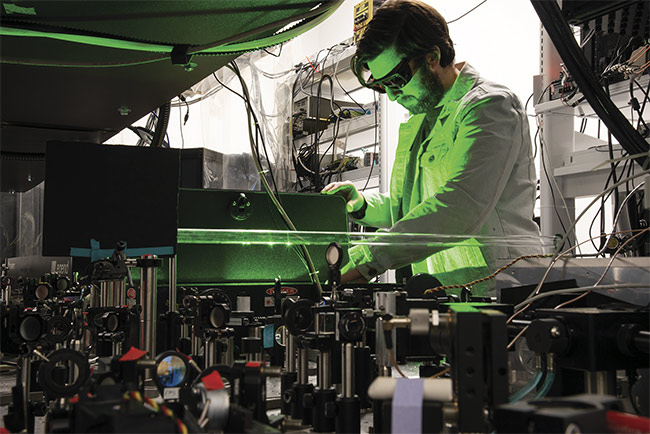
Figure 2. Researcher Seth Lieberman makes adjustments to a laser experiment in the Schaffer-Nishimura Lab at Cornell University. Courtesy of Seth Lieberman/Cornell University.
Schaffer credited Theodore Schwartz, a neurosurgeon at Weill Cornell Medicine, with conceiving of a laser-based approach that improved upon the three-decade-old surgical
procedure called multiple subpial transection, which is still in use and uses a curved needle to produce the interruption of seizure propagation. The new approach is intended to be more precise and less invasive. Schaffer and Lieberman said their group’s next step will be to seek grant funding to build on their success in animal models and to work toward human clinical application.
“We’ve been using an animal model with a flat cortex in our studies to this point, and we are looking to move into a model with a cortex more analogous to a human brain, that has folds (gyri) and indentations (sulci),” Lieberman said. “The idea is we can build a map of how the seizures propagate through the brain and eventually come up with a treatment plan to cut specific lateral connections.”
The researchers want to move beyond using iron chloride in laboratory rats. In the future, Schaffer said, the team wants to move toward a model of traumatic
brain injury, which is a well-recognized cause of seizures and epilepsy.
Schaffer and Lieberman consider their method to be the next logical step in experimentation beyond the current use of thermal ablation to burn or destroy tissue where the seizure foci exist. “Our [pulsed laser] technique is intended to hold onto as much tissue as possible so we can maintain normal functioning,” Lieberman said.
Benefits of ablation
On the other hand, specialists who use ablation — also known as laser interstitial thermal therapy (LITT) — for treating epilepsy indicate that many patients report a profound improvement in their quality of life. Two major, commercially available MRI-guided laser ablation systems are used to treat epilepsy (and also cancer) in health care settings: the Visualase Thermal Therapy System, produced by Medtronic (see illustration image above), and the NeuroBlate System, produced by Monteris. The technologies are similar and, when used on epileptic patients, are intended to burn tissue at the precise location where seizures start. For patients whose epilepsy is drug resistant, doctors use laser ablation to avoid invasive resection surgery, which requires craniotomy. Use of either of these systems requires only a small incision in which a probe is inserted. But there are key differences between the systems.
Visualase uses a 980-nm diode laser with up to 15-W continuous-wave output, whereas NeuroBlate uses a 1064-nm diode laser with up to 12-W pulse mode output. Visualase’s laser is delivered via a 1.65-mm-diameter plastic catheter and diffusing tip fiber. NeuroBlate’s laser is delivered via two probe options: a 3.3-mm-diameter SideFire directional laser probe or a 2.2- or 3.3-mm FullFire diffusing tip probe. Visualase’s tip is cooled by circulating water, and NeuroBlate’s tip is cooled by internalized gas2.
Visualase necrotizes or coagulates soft tissue through interstitial irradiation or thermal therapy using MRI guidance. The system is used in cardiovascular thoracic surgery (excluding surgery involving the heart and the vessels in the pericardial sac); neurosurgery; ear-nose-throat, head and neck, and plastic and general surgery; dermatology; gastroenterology; gynecology; orthopedics; pulmonology; radiology; and urology.
The Visualase system includes four devices: a laser energy source, a cooled laser applicator, a pump for circulating coolant through the applicator, and a computer workstation with MRI analysis software to visualize temperature changes during laser treatment. A 980-nm diode diffusing tip laser is used in the catheter, along with a circulating saline solution that cools the probe throughout the process. The system is used primarily by neurosurgeons.
According to Richard Tyc, vice president of technology and advanced development at Monteris, the NeuroBlate laser delivery probe uses a sapphire tip, which protects the optical fiber, enabling longer laser shots and thus larger ablation zones by using either a diffusing tip fiber or a SideFire fiber. The SideFire probe delivers a more focal output and thus a more directional ablation zone than the diffusion tip probe. The surgeon is guided by a robotic interface and planning software. The probe tip is cooled with CO2 gas to the range of 1 to 14 °C, depending on probe type.
“The robotic component, which is MRI compatible, is attached to the skull bolt,” Tyc said. “The compact diode laser source provides a 1064-nm wavelength at 8- to 12-W output power, and though a lot of people think that [this] wavelength demands an Nd:YAG laser source, it does not. This near-IR wavelength was originally selected due to its low absorption and therefore deep tissue penetration.”
Surgeons are able to easily adapt to the magnetic resonance (MR)-guided system (Figure 3), Tyc said, which was first cleared by the FDA in 2009. In principle, laser ablation for epilepsy begins similarly to a biopsy procedure — the laser delivery probe trajectory is targeted much like a brain biopsy device. But then the procedure shifts to the MRI suite, where the neurosurgeon monitors laser ablation with real-time MR guidance using MR thermometry. Beyond the neurosurgeon, he said, the whole medical team — including neuro-oncologists, epileptologists, and radiation oncologists — needs to be aware of LITT and how it may be used for any given patient. These medical professionals all play a role in the decision to consider using the minimally invasive LITT procedure for a specific case.
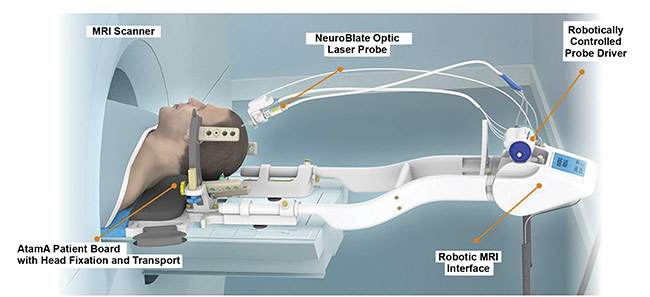
Figure 3. An illustration of the placement of a patient in an MRI scanner while the NeuroBlate system is used for treatment. Courtesy of Monteris.
A study published last year, Tyc said, followed a cohort of 60 drug-resistant epilepsy patients who enrolled as part of a prospective, multicenter study called Laser Ablation of Abnormal Neurological Tissue Using Robotic NeuroBlate System (LAANTERN). Forty-two of the patients reached the one-year follow-up after laser ablation treatment and were given quality-of-life questionnaires. Questions pertained to mobility, self-care, usual activities, pain and discomfort, anxiety and depression, and a visual numerical ranking of the “best possible health state” based on a subjective standard of what the subjects saw as a possible quality of life.
To categorize outcome following surgical treatment, the Engel Epilepsy Surgery Outcome Scale was formalized after the 1992 Palm Desert Conference on Epilepsy Surgery. The classification system is as follows: Class I: seizure free; Class II: seizures occurring rarely; Class III: significant improvement, or prolonged seizure-free intervals; and Class IV: no improvement.
Seizure freedom (Class I) was achieved in 64% of the epilepsy LAANTERN study participants at the one-year mark, and more than 90% experienced pain reduction after ablation3. The study is expected to end in 2027.
Most patients in the study suffered from drug-resistant mesial temporal lobe epilepsy, but the study included other etiologies, such as cortical dysplasia, hypothalamic hamartoma, cavernoma, and tuberous sclerosis. Patients reported minimal pain and discomfort following the procedure, which required short hospitalizations3.
“It’s really about improving people’s quality of life using a minimally invasive technique over open craniotomy,” Tyc said. “That’s what this is all about. And with only a small incision necessary for the 4-mm twist drill hole into the skull for the laser probe, patients often leave the hospital the next day with only a single stitch.”
Chengyuan Wu, M.D., of the Department of Neurological Surgery at the Vickie and Jack Farber Institute for Neuroscience at Thomas Jefferson University has used the Visualase system in many recent procedures. The system’s temperature is set below 43 °C to avoid damaging nearby tissue that is not targeted for ablation.
“Ablation is not a new concept,” Wu said. “For example, radiofrequency ablation has been used on nerve tissue to alleviate pain.”
When he performs laser ablation using Visualase, a stereotactic frame is placed on the patient’s head for the administration of the fiber probe. Then a 3.2-mm drill hole is made in the skull, and the anchor bolt is guided by an alignment rod. The frame is removed once the fiber probe is in place. Once the laser probe is in place, the patient is transferred to an MRI scanner for the duration of the procedure. A low-power pulse is fired first, to confirm that the correct area is being treated. The entire procedure, which uses a 1.6-mm laser applicator (Figure 4), usually takes only a few hours.

Figure 4. A close-up of the Visualase diffusion tip. Courtesy of Medtronic.
A collaborative study that Wu led involved 234 patients from 11 centers who underwent LITT for mesial temporal lobe epilepsy (mTLE) between 2011 and 2017, and for whom follow-up studies had been completed for at least a year. Nearly 60% of the patients achieved seizure freedom4. Ablation cavities were traced with postoperative MRI. The authors of the study concluded that because in subsequent follow-ups this outcome continued toward the two-year mark, LITT had proved to be a viable and successful treatment strategy for mTLE.
Wu is currently working with the same research group to gather longer-term data, he said.
Although the patient’s brain is closely monitored in 3D during this stereotactic procedure, risks still existed, Wu said, such as a loss of peripheral vision. Traditional resection surgery with craniotomy also carries with it greater potential dangers to a patient. But he said the potential benefits to quality of life for those who experience seizure reduction, or even seizure elimination, are hard to ignore.
Another neurosurgeon who has been at the forefront of laser treatment of epilepsy and seizure foci is Peter Warnke, M.D., a professor of neurosurgery and the director of stereotactic and functional neurosurgery at the University of Chicago. His group has participated in more than 300 laser ablations in children and adults.
In a case study published earlier this year, Warnke and his colleagues examined the use of LITT on a 27-year-old man with a nitrogen permease regulator-like 3 (NPRL3) gene mutation, which causes seizures originating from more than one cortical region. The man’s seizures — which caused dizziness, staring, heavy breathing, body stiffening, and shaking — were resistant to pharmaceutical remedies. EEG results showed that he had two independent seizure foci, one in the left hippocampus and one in the left orbitofrontal cortex. His seizures ceased following the LITT procedures using the Visualase system5.
“We were among the first institutions to perform the LITT procedure,” Warnke said. “The limitation on LITT is purely size, as the seizure focus needs to be about 3 cm or less. For a larger epileptic focus, resection is still the best option.”
Prior to the ablation procedure, MRI, PET, and other technologies are used to create a temperature and damage map of the brain to gather data used to help minimize potential harm to sensitive areas.
For cases involving “cataclysmic” epilepsy, Warnke’s team has used Visualase to perform laser hemispherectomy, in which the right and left hemispheres of the brain are disconnected to prevent seizure propagation without affecting other brain functioning. The team has also used the technology for stereotactic laser amygdalohippocampectomy for mTLE patients, in which a portion of the temporal lobe is removed to prevent seizures. In some cases, Warnke said, there may be multiple foci treated with LITT that would be difficult to address using other types of treatment.
“The power and temperature of the system’s laser can be modulated, depending on what we’re trying to accomplish,” Warnke said.
In recent years, Warnke’s center has been involved in a long-term clinical study to measure the effectiveness of the system in reducing and eliminating seizures in patients with mTLE. “We want to see whether we can develop the technology and therapy further,” he said.
Changing the mindset
Despite many successful outcomes, Wu and others involved in laser therapy would like to see more epilepsy patients consider both conventional and laser surgery as an option once they understand the potential benefits. Wu referenced a survey of more than 100 patients that was conducted about a decade ago at the Department of Neurology at SUNY Downstate Medical Center that revealed that more than 50% of the patients said they would not consider brain surgery due to the perceived danger it presented, even if it would guarantee a stop to their seizures6.
The survey concluded that educational efforts were needed to address patients’ concerns, and Wu said such efforts are ongoing.
“There is still a stigma surrounding brain surgery,” he said. “But we’re talking about technology that not only can heal people but can improve their quality of life.”
References
1. S. Nagappan et al. (2019). In vivo femtosecond laser subsurface cortical microtransections attenuate acute rat focal seizures. Cereb Cortex, Vol. 29, Issue 8, pp. 3415-3426.
2. R. Tyc et al. (2020). Magnetic resonance-guided laser interstitial thermal therapy: historical perspectives and overview of the principles of LITT.
In Laser Interstitial Thermal Therapy in Neurosurgery
, V.L. Chiang et al. eds. Springer, www.doi.org/10.1007/978-3-030-48047-9_1.
3. P. Landazuri et al. (2020). A prospective multicenter study of laser ablation for drug resistant epilepsy — one year outcomes. Epilepsy Res, Vol. 167, p. 106473.
4. C. Wu et al. (2019). Effects of surgical targeting in laser interstitial thermal therapy for mesial temporal lobe epilepsy: a multicenter study of 234 patients. Epilepsia,
Vol. 60, Issue 6, pp. 1171-1183.
5. S. Abumurad et al. (2021). Laser interstitial thermal therapy for NPRL3-related epilepsy with multiple seizure foci: a case report. Epilepsy Behav Rep, Vol. 16, p. 100459.
6. N. Prus and A. Grant (2010). Patient beliefs about epilepsy and brain surgery in a multicultural urban population. Epilepsy Behav, Vol. 17, Issue 1, pp. 46-49.
The Epilepsy Foundation Tracks Progress
The Epilepsy Foundation serves as a resource for people with epilepsy and the providers who care for them. It provides information on all current treatment methods for the disorder, including laser-based modalities.
The foundation’s website, www.epilepsy.com, features an “Epilepsy Pipeline Tracker” that tracks the progress of drugs and devices — for treatment and diagnosis — that are currently in development and includes links to various clinical trials. The tracker notes that both the Visualase and NeuroBlate systems have been tested in drug-resistant subjects. It also includes information on methods such as deep brain stimulation and implantable electric arrays.
The website also includes information on treatment options for drug-resistant epilepsy (defined as not responsive to two or more drug regimens). Among these options are resective surgery, metabolic treatment, and immunotherapy. The website notes that the laser ablation procedure may not work for all candidates who qualify for traditional resective surgery.
Jacqueline French, M.D., the foundation’s chief medical and innovation officer, said the organization couldn’t speak to the efficacy of laser-based methods.
“The Epilepsy Foundation does not endorse any one treatment or device,” she said. “We provide information about the various treatment options so that people with epilepsy, their families/caregivers, and their medical team can work together to determine what’s the best treatment for them.”
The organization sponsors clinical trials and posts their results, and it has established digital tools to aid in research. French and members of the foundation’s professional advisory board help to provide “strategic and creative direction,” aligning partnerships between academia, industry, and government as new methods are brought forward.
Although treatments for epilepsy continue to advance, studies indicate that one-third of adults and up to 25% of children with the disorder live with uncontrolled seizures, French said. “If surgery (including laser) renders a patient seizure-free, they can eventually resume driving, and there will likely be other gains regarding employability and social engagement.”
Epilepsy data as of 2015. Courtesy of the CDC.