Recent studies have found that virtual colonoscopy can detect precursors to cancer as well as optical colonoscopy can, but will it replace the optical method?
Hank Hogan, Contributing Editor
For scientists researching ways to prevent death, colon cancer offers a tempting target because screening techniques can spot precancerous tissue, and it is known which part of the population should be checked. And even though benign lesions (known as adenomas) may take up to a decade to become dangerous, there are methods to safely remove them.

A 3-D endoluminal view of a sigmoid villous adenoma is seen in a 60-year-old female undergoing screening via computed tomography colonography. Adenomas greater than 10 mm or with particular attributes are the precursors to colon cancer. This image was derived from CT data using software. All images courtesy of Dr. David H. Kim, University of Wisconsin Medical School.
It all adds up to what should be an easy therapeutic win, noted Dr. David H. Kim, an assistant professor of radiology at the University of Wisconsin Medical School in Madison. “If you look at the molecular parthenogenesis of colon cancer, it is the perfect cancer to prevent.”
Two recent large-scale studies have shown that diagnosticians may have a new tool in this fight. CT colonography, also known as virtual colonoscopy, has been shown to detect potential precursors to cancer as well as optical colonoscopy does.
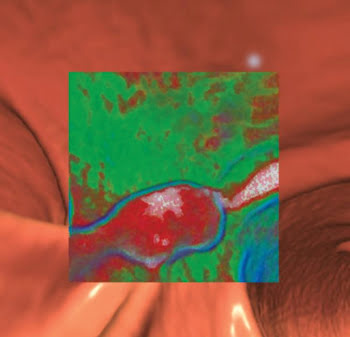
A 3-D endoluminal view of a polyp imaged with CT colonography is shown. A translucency function applied in software (inset) demonstrates the red signature of a soft-tissue polyp.
That’s good news for those seeking to prevent cancer deaths; however, there are some drawbacks to consider. For example, the increased use of CT scans brings risks — such as exposure to ionizing radiation — that must be accounted for and managed. Also, researchers have shown that, despite its less invasive nature, CT colonography may not be preferred to the older optical technique by all segments of the population.
Latest findings
Even though it is easily preventable, colon cancer is the second most common cancer killer in the US. The National Cancer Institute estimates that there were more than 153,000 new colon and rectal cancer cases diagnosed in 2007 and more than 52,000 deaths.
The deaths are attributable to the fact that there are about 80 million people in the US over the age of 50 who should be screened but only 40 million who are being screened, Kim said.
The desire to increase the screening ratio to well over 50 percent is a good part of the impetus behind the development of CT colonography. The traditional screening method, optical colonoscopy, involves a bowel-cleansing preparation, sedation and the insertion of an endoscope through the entire length of the intestines. Suspicious polyps are removed at the time of the screening.
CT colonography, in contrast, doesn’t require sedation or the insertion of an endoscope. Therefore, patients recover faster, and there is no risk of perforating part of the bowel.
The downside is that CT colonography still requires a bowel preparation. The colon also must be inflated, which is performed by pumping a gas through a tube inserted into the rectum. Finally, CT colonography is only diagnostic. If something must be removed, the patient still has to undergo optical colonoscopy, either immediately or at a later date.
Most importantly, there has been some debate about the effectiveness of CT colonography at finding adenomas. A series of studies published in 2003 yielded conflicting results, but two new investigations have produced good results.
Study results positive
The first was published in the New England Journal of Medicine in October, with Kim the lead author. Performed at the University of Wisconsin Medical School, the study compared the effectiveness of CT colonography with that of optical colonoscopy in diagnostic screening programs. Clinicians examined more than 6000 patients, with nearly the same number screened by each method. The patients had no symptoms, were over 50 years of age and were enrolled in one or the other of the screening programs.
Using the two techniques, the researchers found the same number of adenomas —103 — that were 10 mm or greater in size. They found 14 invasive cancers with CT colonography and four with optical colonoscopy. They discovered almost the same percentage of patients with advanced neoplasms — a category that includes all carcinomas — with adenomas greater than 10 mm and with smaller adenomas with specific precancerous attributes. In the CT colonography group, 3.2 percent of the patients had advanced neoplasia while 3.4 percent of the optical colonoscopy patients did.
However, when CT colonography was used, confirming advanced neoplasia required removing far fewer polyps — 561 — than the 2434 removed when optical colonoscopy was used for screening. The optical screening group had seven bowel perforations; the CT colonography group had none.
Kim noted that the end result was the same but that many more polyps were removed by the optical colonoscopists. “They’re taking out a large number of polyps which have little or no malignant potential. So all you’re doing is increasing risk. And that’s borne out by the number of complications between the two programs.”
The second study has yet to be published, although preliminary findings were announced at the American College of Radiology Imaging Network meeting last fall. Fifteen sites took part in the trial, and approximately 2600 people were screened to determine the sensitivity of CT colonography versus optical colonoscopy. The participants underwent the CT procedure and then the optical one on the same day, with the results of the first screen matched against those of the second.
For polyps found by CT, only those confirmed by the optical method were deemed to be true. The preliminary findings indicated that the detection rate for intermediate and large polyps with CT colonography is similar to that with optical colonoscopy.
Although these results are encouraging, those seeking to be screened shouldn’t rush out for a CT colonography, cautioned University of Cincinnati associate professor of medicine Dr. Jonathan Kushner. He noted that the technique is evolving rapidly in terms of hardware, software and procedures. For example, the latest studies use carbon dioxide instead of air to inflate the colon for better results and a more positive patient experience. They also use improved CT technology for a faster scan, requiring patients to hold their breath a shorter time.
Studies have shown that training is critical for accurate CT colonography. Without it, distinguishing a potentially dangerous polyp that should be removed from something benign — or even from fecal matter — can be difficult.
A medical director of an endoscopy unit, Kushner noted that this means there can be varying results from different centers and clinicians when it comes to CT colonography. But he acknowledged that traditional optical colonoscopy isn’t perfect and that it can fail to detect lesions.
In the right hands, the two techniques might be equal or, perhaps, the new approach might be better. However, there are two things that Kushner says should be kept in mind.
The first is that optical colonoscopy technology is advancing, with devices coming online that offer high-definition imaging and more than a 180° range of vision. Other technologies being developed include narrowband imaging, where light of a particular hue is used. A blue source, for example, would enable the colonoscopist to literally see below the surface. There also are optical sectioning techniques such as confocal microscopy being developed for endoscopes. The end result could be the ability to do an almost histological in situ examination of polyps.
The second is that an optical colonoscope is not just a diagnostic tool. It also can remove polyps. Although there is agreement that those measuring 10 mm and above should be removed and those below 5 mm can be left alone, there is no agreement about what to do for the polyps in between. With CT colonography, the doctor and patient have a decision to make with regard to these intermediate polyps: continued screening or removal.
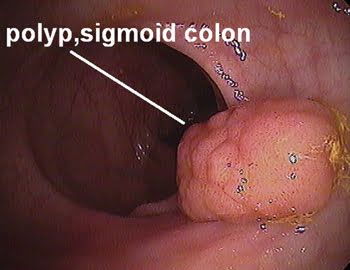
This optical colonoscopy image was taken just before the polyp’s removal.
That’s not the case with the optical approach. “When you’re done, you’re done. There’s little left to be concerned about. The polyps are off, if they were there,” Kushner said.
On the other hand, the chance that a follow-up to CT colonography will be needed at all could be slight. Studies have shown that the majority of patients — 87 percent in the Wisconsin study — do not require any further procedures. However, if a follow-up were needed, that means another bowel preparation, the part of the entire process that most patients dislike the most.
Avoiding an overdose
Everyone who undergoes a CT colonography will be exposed to x-rays, and that has raised some concerns. In a New England Journal of Medicine article published in November 2007, David J. Brenner and Eric J. Hall of Columbia University Medical Center in New York pointed out that the number of CT scans of all varieties is increasing, with more than 60 million a year performed today as compared with about 3 million in 1980. Each scan brings with it some potential for an increased risk of cancer because of exposure to ionizing radiation.
The magnitude of the overall risk is the subject of some debate. Brenner and Hall estimate that perhaps 2 percent of all cancers in the US might be attributable to CT scan exposure. The actual figure depends on the age and gender of the patient, how many times the patient is scanned during a lifetime, and the dose for the various scans. There are unknowns in those factors, although many radiologists contend that the dosage figures used by Brenner and Hall are higher than called for by current standards.
There is also the question of technological and procedural changes over time to consider. For the former, more sensitive detectors may result in lower doses. As for the latter, these show up in programs such as the Image Gently campaign. This is an effort by organizations such as the Society for Pediatric Radiology, the American College of Radiology, the American Society of Radiologic Technologists, the American Association of Physicists in Medicine and others to provide children the correct-size scan and doses as well as frequency.

This CT colonography workstation is used in polyp detection and characterization. The endoluminal view is in the central pane in the middle of the picture. The colonic map showing location is in the upper left corner. Two-dimensional multiplanar images on the right-hand side are for polyp characterization. The workstation allows easy navigation within the 3-D environment and seamless transition into various 2-D reformatted planes for further analysis.
Dr. Donald P. Frush, chief of pediatric radiology at Duke University Medical Center in Durham, N.C., noted that recent data indicate there has been an increase in overall dose over the past few decades, largely because of CT scans and nuclear medicine. New studies have shown that the old assumption that the medical imaging dose is small compared with everything else is no longer valid. “The dose for medical imaging probably is near or may exceed background radiation, according to this data,” Frush said.
However, the downside of increased ionizing radiation exposure resulting from CT colonography must be balanced against the benefits, one of which would be the potentially lifesaving detection of the precursors to colon cancer. Another would be the possibility of uncovering other unsuspected but potentially clinically important problems. Studies have shown that a few percent of those patients undergoing CT colonography have such conditions, with some of those being extracolonic cancers.
Another important factor is the age of the population being screened. Screening occurs in adults over 50, and this age group is not as vulnerable to radiation as children are. If they undergo CT colonography every five or 10 years, they also will be exposed to far fewer scans than would be the case if they were in their 20s.
This assumes that records are complete and travel with patients as they switch from one doctor to the next. It also assumes that the patient remembers how many CT scans he or she has had, which can be problematic after several years have passed. Efforts are under way to develop good dose-recording methods. Many of these, however, are on, at most, a regional and not a national scale.
Patient preferences
Such concerns today are somewhat moot. CT colonography faces some significant hurdles, even granting that it is as good as optical colonoscopy at detecting cancer. For one thing, CT colonography is not covered by most insurance; hence, many people confronted by the need to pay out of pocket might opt for the more traditional screening. The Wisconsin study was made possible, in part, because insurers agreed to pay for CT scans.
Another question is whether the new method substantially improves the screening rate. A study by Roshini C. Rajapaksa, Michael Macari and Edmund J. Bini that appeared in the November 2007 issue of Clinical Gastroenterology and Hepatology indicates that it might not. The group surveyed 272 patients who underwent CT colonography followed by optical colonoscopy. Overall, it found no preference for one procedure over the other, which agrees with some studies but not all.
However, the researchers found that racial and ethnic minorities are significantly less likely than whites to prefer the CT approach over the optical one. They also found that white patients are significantly more willing to undergo CT colonography again than are racial and ethnic minorities. These findings track differences reported in the paper about abdominal pain and embarrassment.
How accurate these results are is somewhat uncertain because most of the participants were men. What’s more, the study was done with CT technology and colonography techniques that are no longer used at most institutions, which could have had an impact. Nonetheless, it does raise questions about the effectiveness of CT colonography at increasing screening rates.
Improved techniques could change this situation. One is prepless CT colonography, which uses software to identify and remove stools and fecal matter from the images. There is some work being done in this regard, although more research and development is needed.