About two-thirds of oral cancer patients live in lower-income regions, which often lack access to adequate health care. Now, smartphone imaging technology aims to tackle the disparity.
RONGGUANG LIANG, UNIVERSITY OF ARIZONA COLLEGE OF OPTICAL SCIENCES
Combined, oral and oropharyngeal squamous cell carcinomas (OSCCs) make up the sixth most common cancer worldwide, accounting for approximately 400,000 new cases each year. The incidence of the disease is often the result of tobacco smoking and chewing, betel quid use, alcohol abuse, and poor oral hygiene.
About two-thirds of OSCCs occur in low- and middle-income regions, including Bangladesh, Malaysia, Nepal, Pakistan, Sri Lanka, Thailand, and Vietnam, which particularly face very high rates. India is another country with high incidence, with the eighth highest age-adjusted death rate of head and neck cancers in the world; among females there, this rate is the highest in the world. The five-year survival rates with OSCCs in these and other lower-income areas range from 10 to 40 percent; in the U.S., this rate is about 62 percent.
While low- and middle-income regions often lack access to adequate health care infrastructure, many of these countries are well-connected by mobile phone networks. These enable low-cost, portable systems that can bring the required specialized care to patients in remote and underserved communities. This includes a system that specifically screens for oral cancers.
Several mobile phone health applications have demonstrated the potential to improve health outcomes and delivery of health services1,2. There is preliminary evidence that use of these mobile imaging systems can increase efficiency of data collection, transmit health information more promptly, improve patient adherence to medications, and enable remote diagnosis2.
The device that screens for oral cancers is a dual-view, dual-modality system based on a smartphone. It was funded by the National Institutes of Health (NIH) and developed by an international team of researchers from the University of Arizona, India’s Mazumdar Shaw Cancer Center, the KLE Society’s Institute of Dental Sciences in India, the University of California Irvine, and Roswell Park Cancer Institute in Buffalo, N.Y.

Figure 1. Dual-view, dual-modality, smartphone-based oral cancer screening system with whole-mouth module (left) and flexible intraoral probe (right).
This screening device features a module that captures whole-mouth, white-light, autofluorescence images and another that captures high-resolution versions of such images over local regions inside the mouth cavity. With a flexible intraoral imaging probe, it can reach even the posterior regions inside the mouth, such as the base of the tongue and tonsils, for oral and oropharyngeal cancer screening.
The whole-mouth imaging module and intraoral imaging probe (Figure 1) present active white-light and blue-light illumination. The images captured with this system (such as those shown in Figure 2) are uploaded to a web server and processed for image enhancement, allowing remote specialists to review the enhanced multimodal images and provide prompt diagnosis.
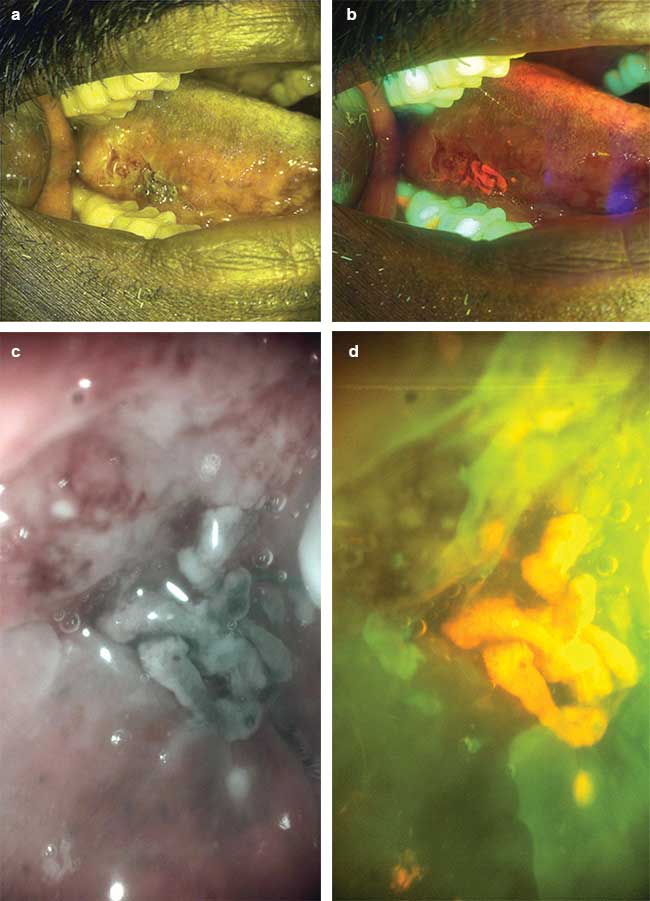
Figure 2. A series of white light (a, c) and autofluorescence (b, d) images captured with the whole-mouth module (a, b) and intraoral probe (c, d).
The system provides high-resolution, dual-imaging modalities for better diagnostic sensitivity and specificity, mobile application for analyzing images and identifying suspicious regions, real-time communication with remote specialists, comprehensive oral cavity examination, and low-cost, easy-to-use portability and durability.
These features highlight the suitability of this technology for oral cancer screening in developing countries. It has the potential to bring much-needed specialty diagnostic services to remote, low-resource regions without the cost and logistic concerns associated with in-person visits.
The largest single variable affecting survival appears to be the cancer’s stage at the patient’s initial visit. However, the reasons for delay in diagnosis of OSCCs are complex and influenced by the patient, providers, infrastructure, and health systems. Diagnosis is often delayed in marginalized at-risk populations living in rural areas with lack of access to primary health care, low health literacy, and poor adherence to referral and follow-up. Other challenges with oral cancer screening programs include poor patient compliance to follow up, slow rates of information transfer after screening, and the lack of a permanent portable record of patients’ medical and oral cavity examination data.
The increase in the number of human papilloma virus-related cancers has posed additional challenges in OSCC detection. Such cancers occur most commonly in the base of the tongue and the tonsillar region of the oropharynx, which are areas not amenable to unaided visual inspection. These also are usually asymptomatic at the early stages and therefore not diagnosed until an advanced stage in neck disease, even when compared to smoking- and alcohol-related head and neck cancers.
This mobile/remote oral screening approach should enable local health care workers to diagnose oral lesions more efficiently and at an earlier stage; it should also facilitate referral to specialists without delay. The new system will eventually reduce costs and improve detection rates, treatment outcomes, and patient quality of life. It is currently undergoing a pilot study in India, with more than 150 patients screened. The results are thus far very encouraging.
Meet the author
Rongguang Liang, Ph.D., is a professor in the University of Arizona’s College of Optical Sciences. His research focuses on optical engineering and new imaging techniques and devices for biomedical applications. Liang is a former principal research scientist at Eastman Kodak Co. He is a SPIE fellow and topical editor of The Optical Society’s journal Optica; email: [email protected].
References
1. https://web.stanford.edu/~manup/Oscan/.
2. Praveen N. Birur et al. (2015). Mobile health application for remote oral cancer surveillance. JADA, Vol. 146, Issue 12, pp. 886-894.